Journal of Otolaryngology and Ophthalmology of Shandong University
2019, 33 (
):
1-11.
10.6040/j.issn.1673-3770.1.2019.011
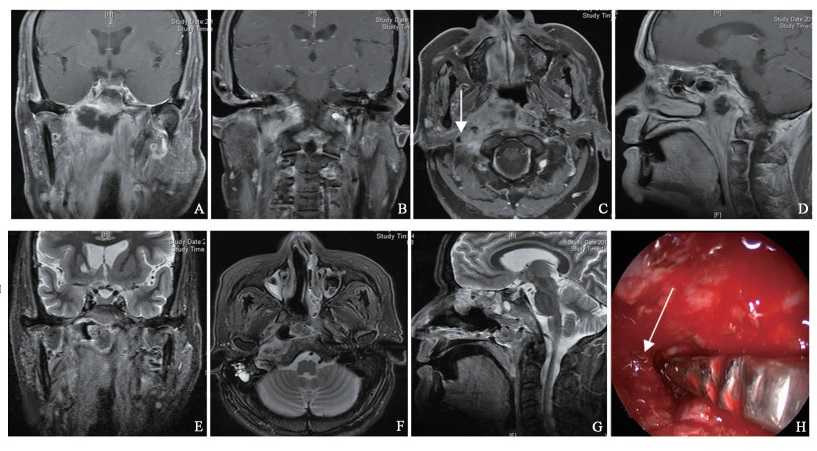
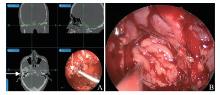
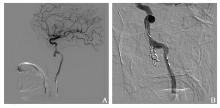
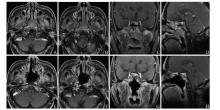
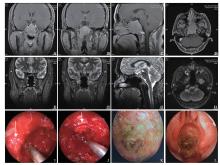
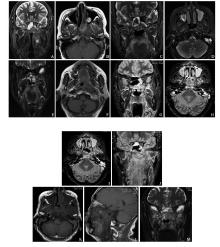
Radiotherapy is the conventional treatment for nasopharyngeal carcinoma. Although the 5-year survival rate has greatly improved, there are still several cases of recurrent or residual nasopharyngeal carcinoma. The treatment principles of recurrent or residual lesions include second-course radiotherapy, chemotherapy, and surgery. The complications following radical radiotherapy and second-course radiotherapy seriously affect the quality of life in patients. The current surgical methods include open surgery and endoscopic surgery. Open surgery can provide a sufficiently open field of operation, but is associated with some serious damage. Endoscopic nasopharyngeal carcinoma resection has been carried out lately, and only few medical institutions in China perform these operations. However, with the emergence of the concept of endoscopic skull base surgery and new medical instruments and equipment, endoscopic nasopharyngeal carcinoma surgery has become a good surgical choice. However, this requires strict surgical indications, skills of endoscopic skull-base surgery, and long-term follow-up.





{kind=link}