ISSN 1673-3770 CN 37-1437/R

|
||||||||||||||||||||||||||||||||||||||||||||||||
|
Types of endoscopic transnasal nasopharyngectomy for nasopharyngeal carcinoma
Journal of Otolaryngology and Ophthalmology of Shandong University
2019, 33 (2):
39-45.
DOI: 10.6040/j.issn.1673-3770.1.2019.016
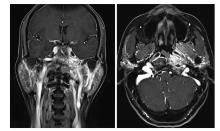
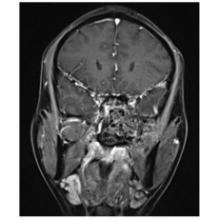
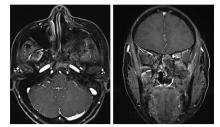
To establish the types of endoscopic endonasal nasopharyngectomy for nasopharyngeal carcinoma (NPC) based on anatomic study and clinical applications. Dissection of the skull base using an endoscopic endonasal approach was performed on a cadaver head. The procedures of endoscopic endonasal nasopharyngectomy for recurrent NPC (rNPC) were used and established. The procedures of endoscopic endonasal nasopharyngectomy for rNPC were grouped into 4 types: type Ⅰ was used for rT1 and rT3 rNPC located in the midline of the nasopharynx and skull base: type Ⅱ was used for rT2 rNPC with involvement of the cartilaginous Eustachian tube, medial petroclival region, and parapharyngeal space: type Ⅲ was used for rT4 rNPC extending further laterally into the lateral petroclival region, infratemporal fossa, middle of the skull base, superior orbital fissure, cavernous sinus, and cranial nerves: and type Ⅳ was used for rNPC invading the internal carotid artery (ICA) and middle cranial fossa. The 4 types of endoscopic endonasal nasopharyngectomy are effective for the surgical treatment of rNPC. Pre-operation evaluation and staged exposure of the ICA is reliable, which will be an effective guideline for surgical treatment of rNPC.
Table 2
Pre-operative scoring of the internal carotid artery involved in nasopharyngeal carcinoma
Extracts from the Article
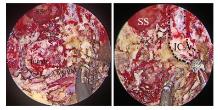
根据病变对ICA累及的程度制定ICA的处理方案尚无统一的规范或指南,本研究团队根据近5年的临床经验,针对病变累及ICA的情况制定了鼻咽癌ICA手术前的评分量表(表2)和鼻咽癌ICA处理的分级策略(表3)。依据鼻咽癌ICA手术前的评分量表确定ICA处理的分级策略,对于3级、4级的ICA分级策咯,术前需行ICA闭塞试验(BOT),若BOT为阴性,可即时行ICA闭塞,术中切除病变组织,对ICA进行咽旁段、岩骨段、破裂孔段和斜坡段进行全程暴露,根据病变侵犯的程度切除相应的ICA;若BOT呈阳性,需行颈外动脉-脑膜中动脉搭桥术,2周后再行rNPC切除,术中切除受累的ICA。
Other Images/Table from this Article
|