ISSN 1673-3770 CN 37-1437/R

山东大学耳鼻喉眼学报 ›› 2019, Vol. 33 ›› Issue (5): 62-68.doi: 10.6040/j.issn.1673-3770.0.2019.177
卢飞燕,卢永田( ),周俊伟,刘渊
),周俊伟,刘渊
Feiyan LU,Yongtian LU(),Junwei ZHOU,Yuan LIU
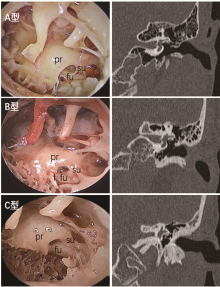
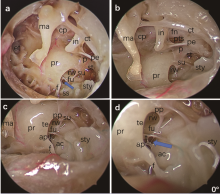
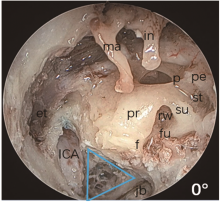
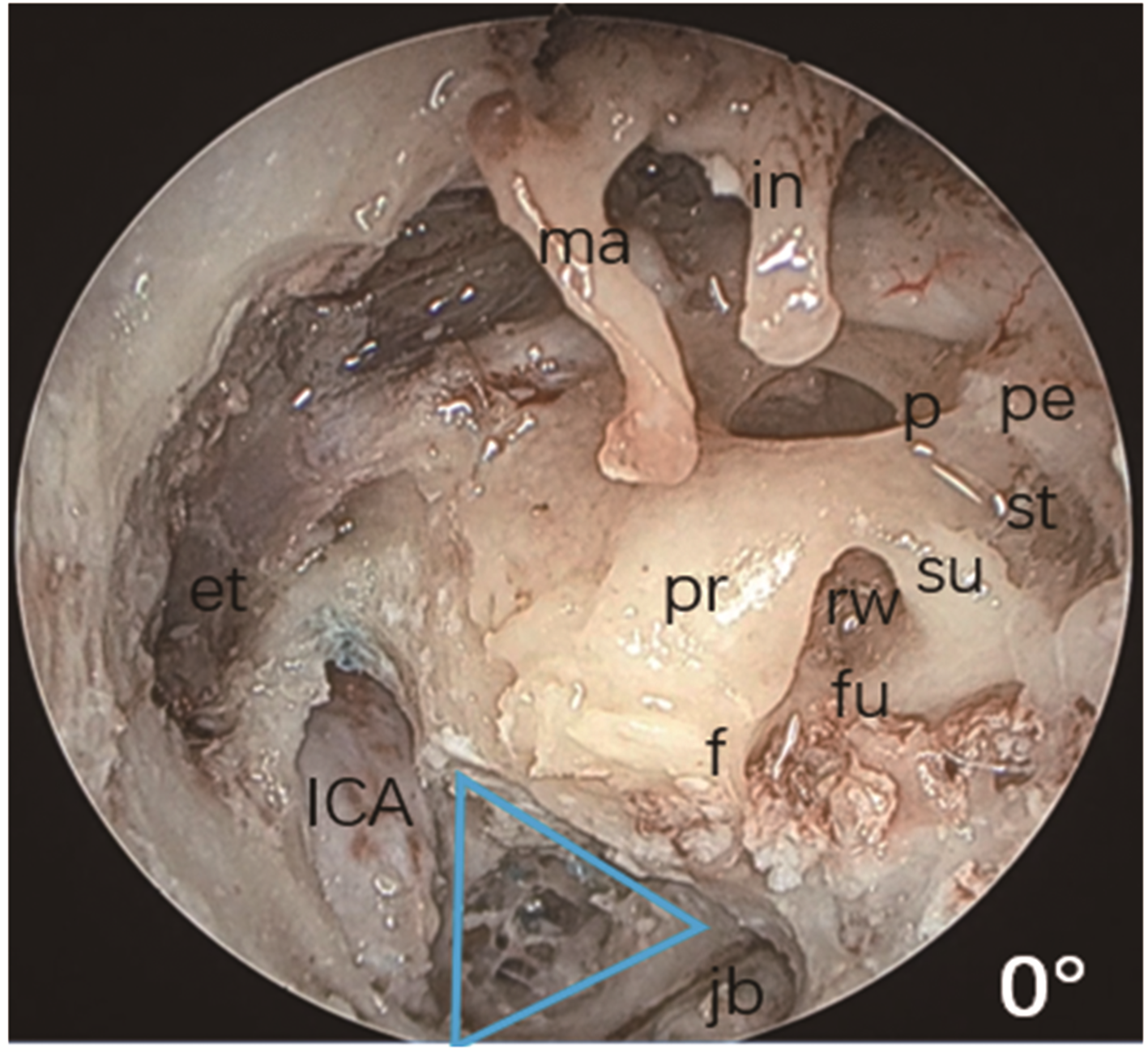
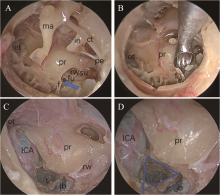
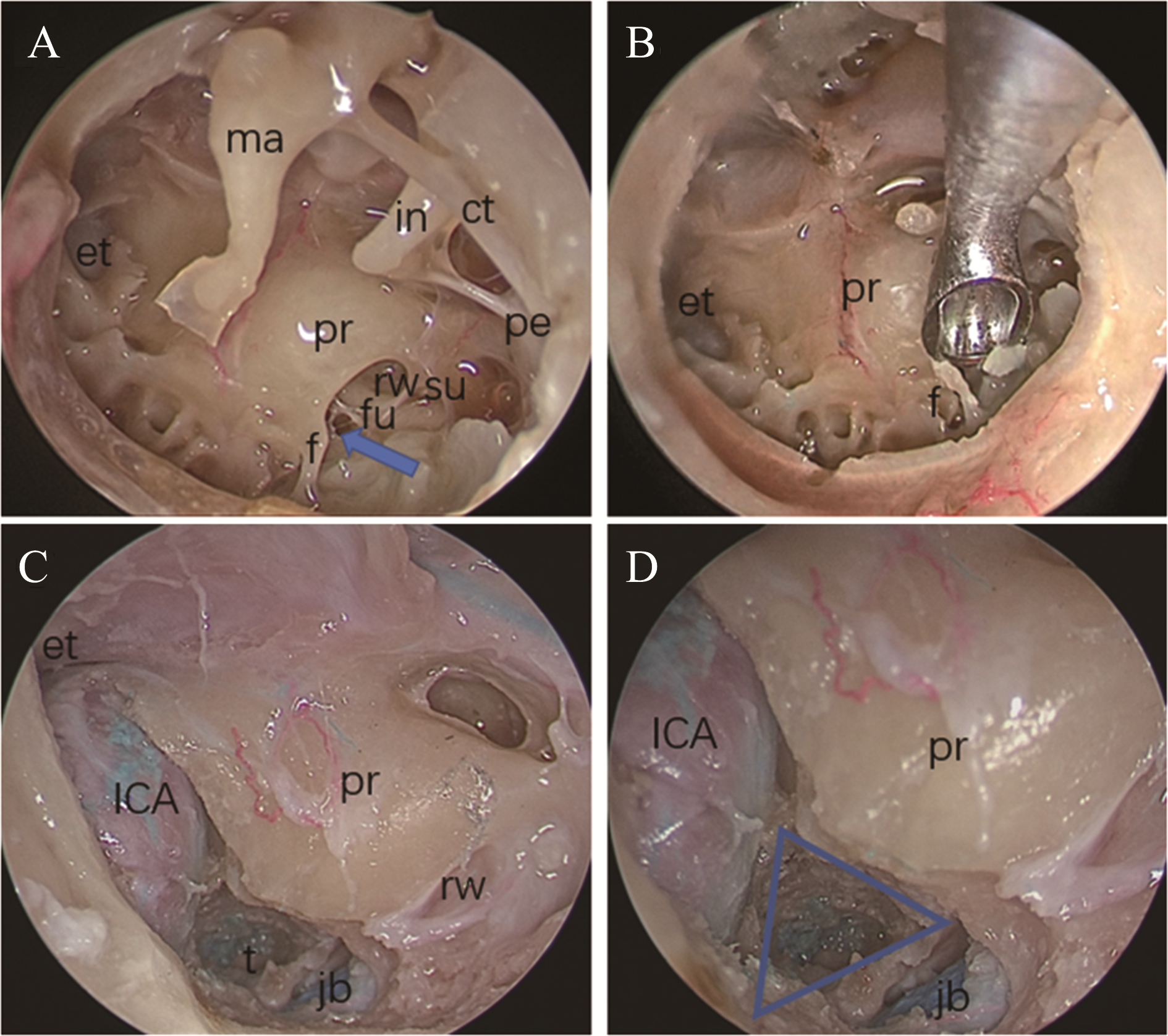
摘要: 探索内镜下经外耳道耳蜗下径路切除岩尖病变的手术入路,观察内镜下后下鼓室及圆窗周围重要的解剖标志,寻找定位耳蜗下通道的解剖标志,同时在高分辨颞骨CT三维重建下量化耳蜗下通道,为该手术入路提供国人恒定的解剖标志及影像学依据。 1.应用10具(20侧)新鲜冰冻成人尸头,模拟内镜下经外耳道耳蜗下径路岩尖气房切除,寻找定位耳蜗下通道的解剖标志;术前在颞骨CT上分别测量耳蜗底转至颈内动脉与颈静脉球夹角之间的距离,以及耳蜗底转至颈静脉球之间的距离。2.回顾性阅读分析85例患者(170侧)颞骨高分辨CT,记录耳蜗下通道与岩尖气房在颞骨CT上的影像学特征,归类其分型情况。 1.20侧冰鲜尸头以及170侧临床患者颞骨CT测量:耳蜗底转至颈内动脉与颈静脉球夹角之间的距离分别为(6.46±1.02)mm、(6.83±1.50)mm;耳蜗底转至颈静脉球之间的距离分别为(3.67±0.58)mm、(3.82±1.29)mm,其中,耳蜗底转至颈内动脉与颈静脉球夹角之间的距离:气化型岩尖分别为(6.79±0.60)mm、(7.19±1.44)mm,非气化型岩尖分别为(6.28±1.17)mm、(6.68±1.50)mm;耳蜗底转至颈静脉球的距离:气化型岩尖分别为(4.06±0.36)mm、(4.06±1.42)mm, 非气化型分别为(3.45±0.58)mm、(3.74±1.22)mm。2.耳蜗下通道与颞骨岩尖气房CT分型:A型气化型31.18%(53耳),B型板障型57.65%(98耳),C型硬化型11.18%(19耳)。 高分辨颞骨CT可作为内镜下经外耳道耳蜗下径路岩尖病变切除的术前重要参考。从解剖学的角度,内镜下经外耳道耳蜗下径路切除岩尖病变是可行的,能够避免损伤内听道、耳蜗、迷路,保存听力,可作为临床治疗上岩尖后下部分较小病变的重要术式之一。
中图分类号:
| 1 | 王若雅 . 颞骨岩部胆脂瘤外科手术治疗及面神经功能保护的临床研究[D]. 北京: 中国人民解放军医学院, 2014. |
| 2 | 汪照炎,王武庆 . 耳内镜外科学[M]. 西安:世界图书出版西安有限公司, 2018: 345-347. |
| 3 |
Marchioni D , Alicandri-Ciufelli M , Pothier DD , et al . The round window region and contiguous areas: endoscopic anatomy and surgical implications[J]. Eur Arch Otorhinolaryngol, 2015, 272(5): 1103-1112. doi:10. 1007/s00405-014-2923-8 .
doi: 10. 1007/s00405-014-2923-8 |
| 4 |
Thomassin JM , Korchia D , Doris JM . Endoscopic-guided otosurgery in the prevention of residual cholesteatomas[J]. Laryngoscope, 1993, 103(8): 939-943. doi:10. 1288/00005537-199308000-00021 .
doi: 10. 1288/00005537-199308000-00021 |
| 5 | Sanna M , Zini C , Gamoletti R , et al . Petrous bone cholesteatoma[J]. Skull Base Surg, 1993, 3(4): 201-213. PMID: 17170912doi:101055/s-2008-1060585 |
| 6 |
Sanna M , Pandya Y , Mancini F , et al . Petrous bone cholesteatoma: classification, management and review of the literature[J]. Audiol Neurootol, 2011, 16(2): 124-136. doi:10.1159/000315900 .
doi: 10.1159/000315900 |
| 7 |
田广永, 徐达传, 黄德亮, 等 . 经迷路下径路切除岩尖病变显微解剖学[J]. 中国耳鼻咽喉头颈外科, 2008, 15(1): 37-39. doi:10.3969/j.issn.1672-7002.2008.01.013 .
doi: 10.3969/j.issn.1672-7002.2008.01.013 |
|
TIAN Guangyong , XU Dachuan , HUANG Deliang , et al . Anatomy of the infralabyrinthine approach to the petrous apex[J]. Chinese Archiver of Otolaryngology-Head and Neck Surgery, 2008, 15(1): 37-39. doi:10.3969/j.issn.1672-7002.2008.01.013 .
doi: 10.3969/j.issn.1672-7002.2008.01.013 |
|
| 8 |
Leung R , Samy RN , Leach JL , et al . Radiographic anatomy of the infracochlear approach to the petrous apex for computer-assisted surgery[J]. Otol Neurotol, 2010, 31(3): 419-423. doi:10.1097/MAO.0b013e3181c99524 .
doi: 10.1097/MAO.0b013e3181c99524 |
| 9 |
Scopel TF , Fernandez-Miranda JC , Pinheiro-Neto CD , et al . Petrous apex cholesterol granulomas: endonasal versus infracochlear approach[J]. Laryngoscope, 2012, 122(4): 751-761. doi:10.1002/lary.22448 .
doi: 10.1002/lary.22448 |
| 10 |
Marchioni D , Alicandri-Ciufelli M , Rubini A , et al . Endoscopic transcanal corridors to the lateral skull base: Initial experiences[J]. Laryngoscope, 2015, 125(Suppl 5): S1-13. doi:10.1002/lary.25203 .
doi: 10.1002/lary.25203 |
| 11 |
朱琳, 张德军, 管国芳, 等 . 显微镜联合耳内镜手术治疗岩尖巨大胆脂瘤一例[J]. 山东大学耳鼻喉眼学报, 2016, 30(6): 101-103,106. doi:10.6040/j.issn.1673-3770.0.2016.345 .
doi: 10.6040/j.issn.1673-3770.0.2016.345 |
|
ZHU Lin , ZHANG Dejun , GUAN Guofang , et al . Treatment of huge cholesteatoma in the petrous apex by microscope combined with otoendoscope: report of 1 case[J]. Journal of Otolaryngology and Ophthalmology of Shandong University, 2016, 30(6): 101-103,106. doi:10.6040/j.issn.1673-3770.0.2016.345 .
doi: 10.6040/j.issn.1673-3770.0.2016.345 |
|
| 12 |
Wick CC , Hansen AR , Kutz JW Jr , et al . Endoscopic infracochlear approach for drainage of petrous apex cholesterol granulomas: a case series[J]. Otol Neurotol, 2017, 38(6): 876-881. doi:10.1097/MAO.0000000000001422.
doi: 10.1097/MAO.0000000000001422. |
| 13 |
Anschuetz L , Presutti L , Schneider D , et al . Quantitative analysis of surgical freedom and area of exposure in minimal-invasive transcanal approaches to the lateral skull base[J]. Otol Neurotol, 2018, 39(6): 785-790. doi:10.1097/MAO.0000000000001827 .
doi: 10.1097/MAO.0000000000001827 |
| 14 |
Kempfle JS , Fiorillo B , Kanumuri VV , et al . Quantitative imaging analysis of transcanal endoscopic Infracochlear approach to the internal auditory canal[J]. Am J Otolaryngol, 2017, 38(5): 518-520. doi:10.1016/j.amjoto.2017.03.01 .
doi: 10.1016/j.amjoto.2017.03.01 |
| 15 |
Trakimas DR , Kempfle JS , Reinshagen KL , et al . Transcanal endoscopic infracochlear vestibular neurectomy: A pilot cadaveric study[J]. Am J Otolaryngol, 2018, 39(6): 731-736. doi:10.1016/j.amjoto. 2018. 07. 024 .
doi: 10.1016/j.amjoto. 2018. 07. 024 |
| 16 |
Jacob CE , Rupa V . Infralabyrinthine approach to the petrous apex[J]. Clin Anat, 2005, 18(6): 423-427. doi:10.1002/ca.20156 .
doi: 10.1002/ca.20156 |
| 17 |
Marchioni D , Alicandri-Ciufelli M , Piccinini A , et al . Inferior retrotympanum revisited: an endoscopic anatomic study[J]. Laryngoscope, 2010, 120(9): 1880-1886. doi:10.1002/lary.20995 .
doi: 10.1002/lary.20995 |
| 18 |
Marchioni D , Alicandri-Ciufelli M , Grammatica A , et al . Pyramidal eminence and subpyramidal space: an endoscopic anatomical study[J]. Laryngoscope, 2010, 120(3): 557-564. doi:10.1002/lary.20748 .
doi: 10.1002/lary.20748 |
| [1] | 冯剑,周涵,董伟达. 喉癌内镜诊断技术研究进展[J]. 山东大学耳鼻喉眼学报, 2019, 33(3): 129-133. |
| [2] | 万文锦,闫玉洁,黎娜,郭人毓,袁慧. 综合护理干预对鼻内镜鼻窦手术后口干症的改善效果观察[J]. 山东大学耳鼻喉眼学报, 2019, 33(3): 134-137. |
| [3] | 何健,钱立庭,高劲. 外耳道腺样囊性癌侵犯中耳、颞叶且伴颈部淋巴结转移一例报告[J]. 山东大学耳鼻喉眼学报, 2018, 32(6): 109-111. |
| [4] | 周鹏,苏开明. 功能性鼻整形解剖学基础及进展[J]. 山东大学耳鼻喉眼学报, 2018, 32(1): 37-41. |
| [5] | 王登元,陈智斌,陈若希,赵晓埝,刘丞. 外耳道胆脂瘤的临床特征及疗效评估[J]. 山东大学耳鼻喉眼学报, 2017, 31(5): 62-66. |
| [6] | 沈莉. 碳酸氢钠联合氟康唑注射液治疗真菌性外耳道炎35例[J]. 山东大学耳鼻喉眼学报, 2016, 30(6): 22-23. |
| [7] | 周鹏,神平,刘稳,李培华,李红权. 药物诱导睡眠内镜检查结果与低氧血症相关性研究[J]. 山东大学耳鼻喉眼学报, 2016, 30(5): 54-57. |
| [8] | 谢畅,颜滨,李建兴,卢永田. 内镜经口入路寰枢椎解剖及临床可行性研究[J]. 山东大学耳鼻喉眼学报, 2016, 30(3): 47-51. |
| [9] | 吕正华. 喉返神经减压术[J]. 山东大学耳鼻喉眼学报, 2016, 30(2): 17-19. |
| [10] | 王刚, 胡金旺, 陶伟, 吴长松, 卫平存. 泪囊在鼻内镜泪囊鼻腔造口术中的解剖学研究及临床应用[J]. 山东大学耳鼻喉眼学报, 2015, 29(6): 26-28. |
| [11] | 朱江彬, 孙秀芹, 南兵卫, 郝宗生. 5%碳酸氢钠液与制霉菌素片混合制剂纱条治疗真菌性外耳道炎156例[J]. 山东大学耳鼻喉眼学报, 2015, 29(6): 82-83. |
| [12] | 何本超, 徐必生, 胡晶, 陈绪清, 王宇. 经扁桃体前外侧进路内镜辅助下茎突截短术15例[J]. 山东大学耳鼻喉眼学报, 2015, 29(4): 58-59. |
| [13] | 李萍. 鼻内镜下单极电凝治疗成人难治性鼻出血102例[J]. 山东大学耳鼻喉眼学报, 2015, 29(4): 88-89. |
| [14] | 黄雄超, 廖首本, 董仕婷, 钟海建, 覃永前. 氟康唑注射液耳浴治疗真菌性外耳道炎71例[J]. 山东大学耳鼻喉眼学报, 2015, 29(3): 29-30. |
| [15] | 杨美艳. 复方黄柏液联合曲咪新乳膏治疗外耳道湿疹40例[J]. 山东大学耳鼻喉眼学报, 2015, 29(2): 20-23. |
|
||