ISSN 1673-3770 CN 37-1437/R

山东大学耳鼻喉眼学报 ›› 2019, Vol. 33 ›› Issue (3): 106-110.doi: 10.6040/j.issn.1673-3770.1.2019.018
陈慧君,宋圣花,周涵( ),董伟达,乔明哲,陈曦,徐进,林子萍,邢光前()
),董伟达,乔明哲,陈曦,徐进,林子萍,邢光前()
Huijun CHEN,Shenghua SONG,Han ZHOU(),Weida DONG,Mingzhe QIAO,Xi CHEN,Jin XU,Ziping LIN,Guangqian XING()
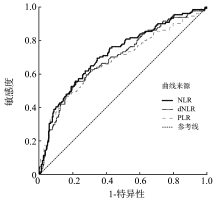
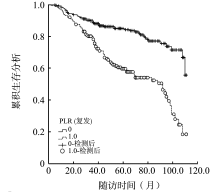
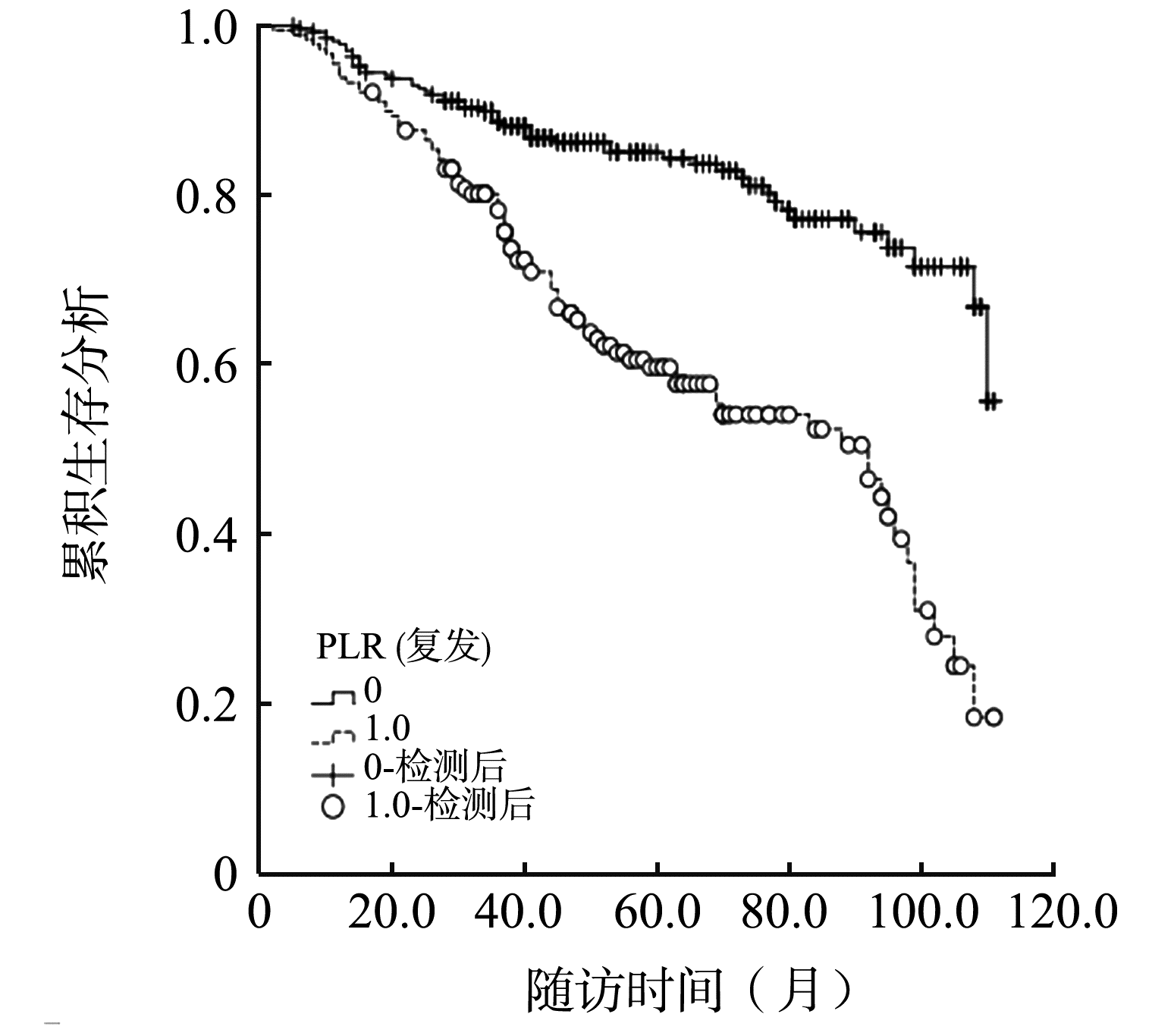
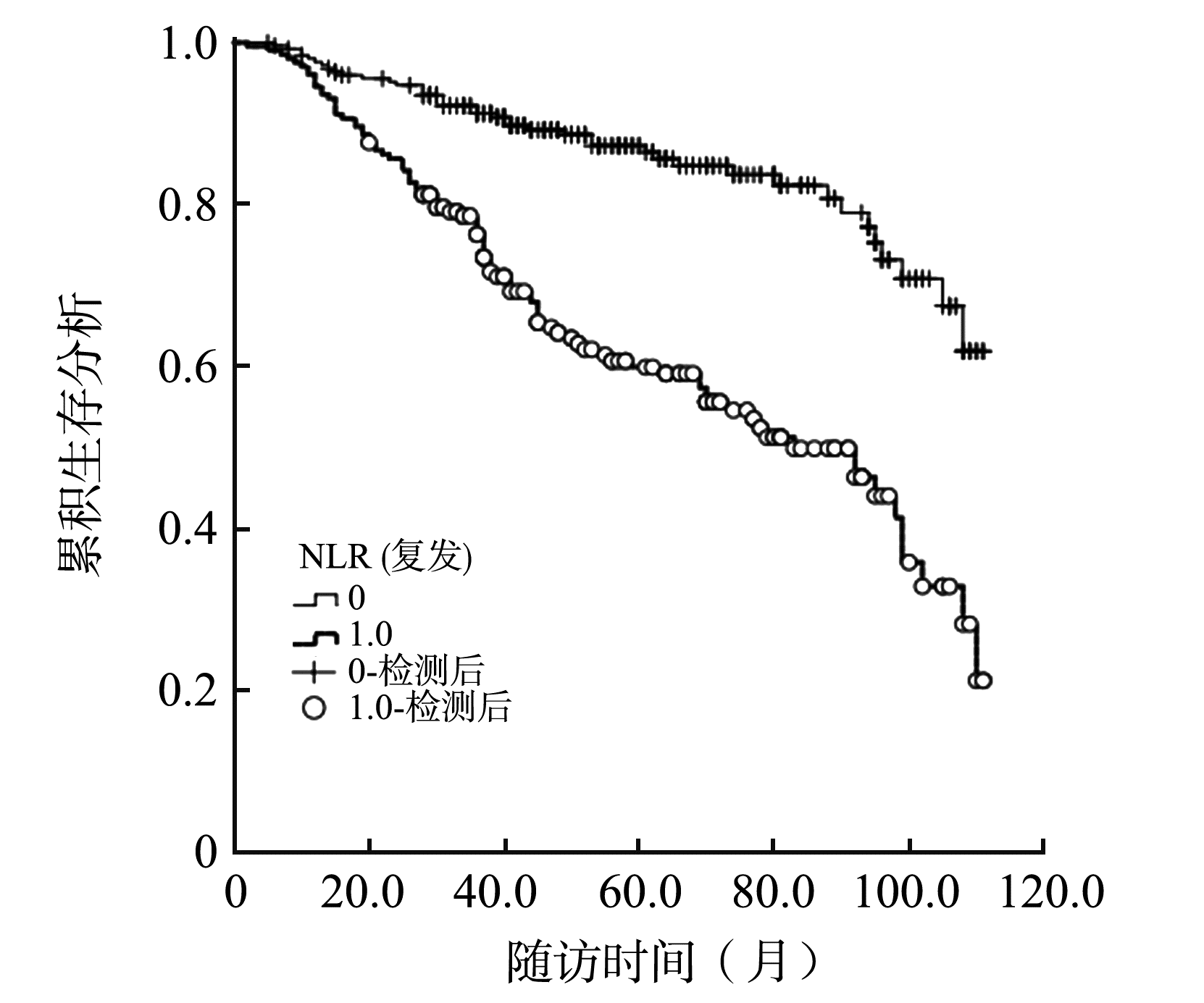
摘要: 探讨术前外周血血小板与淋巴细胞比值(PLR)、中性粒细胞与淋巴细胞比值(NLR)、衍生中性粒细胞与淋巴细胞比值(dNLR)对喉鳞状细胞癌患者复发的影响和预测价值。 回顾性分析南京医科大学第一附属医院473例行初次手术治疗的喉鳞状细胞癌患者的临床资料。根据患者术前的PLR、NLR和dNLR,绘制诊断肿瘤复发的受试者工作特征曲线(ROC),确定PLR、NLR和dNLR界值,从而分成相应的低比值组和高比值组;并采用 Kaplan-Meier分析、COX风险模型分析PLR、NLR、dNLR以及其他临床病理参数与喉癌复发的关系。 PLR、NLR和dNLR诊断肿瘤复发的ROC曲线下面积(AUC)分别为0.683、0.720和0.696。单因素分析显示: PLR、NLR、dNLR、分型、分期、病理分化程度、甲状软骨板累及、淋巴结转移、年龄、凝血功能与喉鳞状细胞癌患者的复发有关;COX风险模型显示: PLR、分型、年龄是影响喉鳞状细胞癌复发的独立危险因素。 术前PLR高的喉鳞状细胞癌患者术后容易复发,PLR对复发的预测价值优于NLR和dNLR,可作为评估喉癌患者预后的重要指标。
中图分类号:
| 1 | 黄选兆, 汪吉宝, 孔维佳. 实用耳鼻咽喉头颈外科学[M]. 北京: 人民卫生出版社,2008:488. |
| 2 |
FengJF, HuangY, ChenQX. Preoperative platelet lymphocyte ratio (PLR) is superior to neutrophil lymphocyte ratio (NLR) as a predictive factor in patients with esophageal squamous cell carcinoma[J]. World J Surg Oncol, 2014, 12: 58. doi:10.1186/1477-7819-12-58.
doi: 10.1186/1477-7819-12-58 |
| 3 |
IshizukaM, NagataH, TakagiK, et al. Combination of platelet count and neutrophil to lymphocyte ratio is a useful predictor of postoperative survival in patients with colorectal cancer[J]. Br J Cancer, 2013, 109(2): 401-407. doi:10.1038/bjc.2013.350.
doi: 10.1038/bjc.2013.350 |
| 4 |
RussoA, FranchinaT, RicciardiGRR, et al. Baseline neutrophilia, derived neutrophil-to-lymphocyte ratio (dNLR), platelet-to-lymphocyte ratio (PLR), and outcome in non small cell lung cancer (NSCLC) treated with Nivolumab or Docetaxel[J]. J Cell Physiol, 2018, 233(10): 6337-6343. doi:10.1002/jcp.26609.
doi: 10.1002/jcp.26609 |
| 5 |
KangMY, JeongCW, KwakC, et al. Preoperative neutrophil-lymphocyte ratio can significantly predict mortality outcomes in patients with non-muscle invasive bladder cancer undergoing transurethral resection of bladder tumor[J]. Oncotarget, 2017, 8(8): 12891-12901. doi:10. 18632/oncotarget.14179.
doi: 10. 18632/oncotarget.14179 |
| 6 |
SabrkhanyS, GriffioenAW, Oude EgbrinkMG. The role of blood platelets in tumor angiogenesis[J]. Biochim Biophys Acta, 2011, 1815(2): 189-196. doi:10.1016/j.bbcan. 2010.12.001.
doi: 10.1016/j.bbcan. 2010.12.001 |
| 7 |
MantovaniA, AllavenaP, SicaA, et al. Cancer-related inflammation[J]. Nature, 2008, 454(7203): 436-444. doi:10.1038/nature07205.
doi: 10.1038/nature07205 |
| 8 |
GrenaderT, NashS, PlotkinY, et al. Derived neutrophil lymphocyte ratio may predict benefit from cisplatin in the advanced biliary cancer: the ABC-02 and BT-22 studies[J]. Ann Oncol, 2015, 26(9): 1910-1916. doi:10.1093/annonc/mdv253.
doi: 10.1093/annonc/mdv253 |
| 9 |
KucharczykJ, SullivanC, LuJ, et al. Prognostic and predictive value of pretreatment derived neutrophil-to-lymphocyte ratio in non-small-cell lung cancer patients treated with an immune checkpoint inhibitor[J]. JCT, 2018, 9(1): 23-34. doi:10.4236/jct.2018.91004.
doi: 10.4236/jct.2018.91004 |
| 10 |
DiricanA, KucukzeybekBB, AlacaciogluA, et al. Do the derived neutrophil to lymphocyte ratio and the neutrophil to lymphocyte ratio predict prognosis in breast cancer?[J]. Int J Clin Oncol, 2015, 20(1): 70-81. doi:10.1007/s10147-014-0672-8.
doi: 10.1007/s10147-014-0672-8 |
| 11 |
EthierJL, DesautelsD, TempletonA, et al. Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: a systematic review and meta-analysis[J]. Breast Cancer Res, 2017, 19(1): 2. doi:10.1186/s13058-016-0794-1.
doi: 10.1186/s13058-016-0794-1 |
| 12 |
ChenL, ZhangF, ShengXG, et al. Peripheral platelet/lymphocyte ratio predicts lymph node metastasis and acts as a superior prognostic factor for cervical cancer when combined with neutrophil: lymphocyte[J]. Medicine (Baltimore), 2016, 95(32): e4381. doi:10.1097/MD. 000-0000000004381.
doi: 10.1097/MD. 000-0000000004381 |
| 13 |
JainS, HarrisJ, WareJ. Platelets: linking hemostasis and cancer[J]. Arterioscler Thromb Vasc Biol, 2010, 30(12): 2362-2367. doi:10.1161/ATVBAHA.110.207514.
doi: 10.1161/ATVBAHA.110.207514 |
| 14 | SuzukiK, AiuraK, UedaM, et al. The influence of platelets on the promotion of invasion by tumor cells and inhibition by antiplatelet agents[J]. Pancreas, 2004, 29(2): 132-140. |
| [1] | 潘晓菲,王军,肖洋,马丽晶. LncRNA CTB-147C22.8对复发性呼吸道乳头状瘤细胞侵袭的影响[J]. 山东大学耳鼻喉眼学报, 2019, 33(4): 66-70. |
| [2] | 黄河,欧阳晖. 下咽癌共病食管癌的高危因素及预后分析[J]. 山东大学耳鼻喉眼学报, 2019, 33(4): 82-86. |
| [3] | 赵青,周涵,殷敏,冯剑,张佳程,刘雅琴,沈宇杰,林子萍,董伟达. 鼻咽纤维血管瘤术前超选择性血管栓塞的应用价值[J]. 山东大学耳鼻喉眼学报, 2019, 33(3): 100-105. |
| [4] | 张佳程,张立庆,周涵,陆美萍,许万云,沈宇杰,刘雅琴,殷敏,董伟达. 鼻腔鼻窦恶性黑色素瘤23例临床分析[J]. 山东大学耳鼻喉眼学报, 2019, 33(3): 95-99. |
| [5] | 姜彦. 鼻咽癌复发及鼻内镜外科手术的应用[J]. 山东大学耳鼻喉眼学报, 2019, 33(2): 1-11. |
| [6] | 陈冬平,杨致欢,张炎,方楠,齐斌. 复发鼻咽癌手术治疗地位的思考[J]. 山东大学耳鼻喉眼学报, 2019, 33(2): 12-16. |
| [7] | 徐文瑞,姜彦. 复发鼻咽癌挽救性手术方法研究进展[J]. 山东大学耳鼻喉眼学报, 2019, 33(2): 35-38. |
| [8] | 刘传合. 我国儿童哮喘患病与诊治现状[J]. 山东大学耳鼻喉眼学报, 2019, 33(1): 28-32. |
| [9] | 雷文斌,刘其洪. CO2激光手术治疗复发性呼吸道乳头状瘤[J]. 山东大学耳鼻喉眼学报, 2018, 32(6): 8-12. |
| [10] | 刘晓静,王愿,张立庆,冯剑,赵青,宋圣花,周涵,董伟达. 鼻窦骨纤维异常增殖症36例临床分析[J]. 山东大学耳鼻喉眼学报, 2018, 32(2): 73-78. |
| [11] | 吕丹,李明霞,马兰枝,张馨元,肖浩,陈飞,刘均,李珍. 累及纵膈的头颈部丛状I型神经纤维瘤病两例[J]. 山东大学耳鼻喉眼学报, 2018, 32(1): 82-86. |
| [12] | 伦杰,张亚楠. 慢性鼻-鼻窦炎伴鼻息肉复发的相关影响因素分析[J]. 山东大学耳鼻喉眼学报, 2017, 31(3): 80-83. |
| [13] | 包伟晶,宁佳羽,朱忠寿,魏日富,林昶. CO2激光切除累及前联合的早期声门癌26例[J]. 山东大学耳鼻喉眼学报, 2016, 30(5): 101-105. |
| [14] | 贾岩峰,杨春伟,宋富春,杨相立,王林,刘吉祥. CO2激光联合质子泵抑制剂治疗复发性声带突肉芽肿的疗效观察[J]. 山东大学耳鼻喉眼学报, 2016, 30(5): 106-109. |
| [15] | 马荣峰,朱富高,孙美红,付涛,张晓恒,曹琳. 突发性聋预后的相关因素分析及疗程选择[J]. 山东大学耳鼻喉眼学报, 2016, 30(4): 69-74. |
|