
ISSN 1673-3770 CN 37-1437/R

|
 Flesh plaque hyperplasia and scar evolution after surgery
Flesh plaque hyperplasia and scar evolution after surgery Intraoperative image of electronic laryngoscope
Intraoperative image of electronic laryngoscope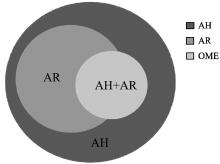 The relationship among adenoidal hypertrophy (AH), allergic rhinitis (AR) and otitis media with effusion (OME)
The relationship among adenoidal hypertrophy (AH), allergic rhinitis (AR) and otitis media with effusion (OME) The left one provides an illustration of "Integration of upper and lower airways". If we add our "lateral airway" into the regular pattern, we'll end up with the following updated diagram calling "Integration of upper, lower and lateral airways"
The left one provides an illustration of "Integration of upper and lower airways". If we add our "lateral airway" into the regular pattern, we'll end up with the following updated diagram calling "Integration of upper, lower and lateral airways"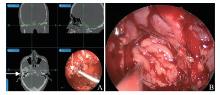 Electromagnetic navigation map of recurrent nasopharyngeal carcinoma
Electromagnetic navigation map of recurrent nasopharyngeal carcinoma Resection steps and resection range of right nasopharyngeal carcinoma
Resection steps and resection range of right nasopharyngeal carcinoma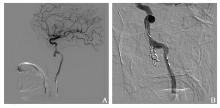 Repeated hemorrhages in the nasal cavity after radical radiotherapy for nasopharyngeal carcinoma
Repeated hemorrhages in the nasal cavity after radical radiotherapy for nasopharyngeal carcinoma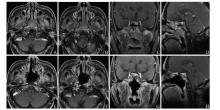 A 62-year-old man relapsed 3 months after undergoing radiotherapy for nasopharyngeal carcinoma, and was diagnosed with poorly differentiated squamous cell carcinoma (T3N0M0). Surgical treatment was performed in May 2015 without chemotherapy nor radiotherapy, with no recurrence after 45 months of follow-up
A 62-year-old man relapsed 3 months after undergoing radiotherapy for nasopharyngeal carcinoma, and was diagnosed with poorly differentiated squamous cell carcinoma (T3N0M0). Surgical treatment was performed in May 2015 without chemotherapy nor radiotherapy, with no recurrence after 45 months of follow-up A 58-year-old woman with non-keratinized undifferentiated carcinoma (T1N0M0) underwent endoscopic surgery for nasopharyngeal carcinoma in August 2014 and postoperative radiotherapy 5 000 cGy/25 f with follow-up till date
A 58-year-old woman with non-keratinized undifferentiated carcinoma (T1N0M0) underwent endoscopic surgery for nasopharyngeal carcinoma in August 2014 and postoperative radiotherapy 5 000 cGy/25 f with follow-up till date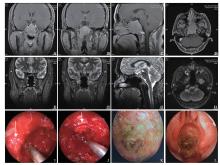 A 38-year-old man with differentiated non-keratinized carcinoma (T3N0M0) underwent endoscopic surgical resection, postoperative radiotherapy, and chemotherapy (DT: 7 623 cGy/33 f, only 25 times; 3 675 cGy/15 f; TP: docetaxel 140 mg/dl + nedaplatin 140 mg/dl), with follow-up for 48 months
A 38-year-old man with differentiated non-keratinized carcinoma (T3N0M0) underwent endoscopic surgical resection, postoperative radiotherapy, and chemotherapy (DT: 7 623 cGy/33 f, only 25 times; 3 675 cGy/15 f; TP: docetaxel 140 mg/dl + nedaplatin 140 mg/dl), with follow-up for 48 months A 48-year-old man with local recurrence of nasopharyngeal carcinoma, 2 years after radiotherapy, refused two-way radiotherapy and underwent total endoscopic resection of the nasopharyngeal carcinoma and postoperative chemotherapy, with a 24-month follow-up
A 48-year-old man with local recurrence of nasopharyngeal carcinoma, 2 years after radiotherapy, refused two-way radiotherapy and underwent total endoscopic resection of the nasopharyngeal carcinoma and postoperative chemotherapy, with a 24-month follow-up A man with nasopharyngeal carcinoma showed recurrence, skull necrosis, liquefaction necrosis in the eustachian tube area, intractable headache, mouth and nose odor (white arrow refers to the exposed internal carotid artery), 6 months after the first radical radiotherapy
A man with nasopharyngeal carcinoma showed recurrence, skull necrosis, liquefaction necrosis in the eustachian tube area, intractable headache, mouth and nose odor (white arrow refers to the exposed internal carotid artery), 6 months after the first radical radiotherapy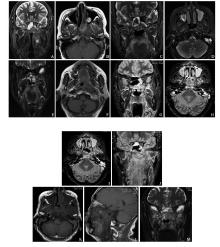 A 58-year-old woman underwent radical radiotherapy for nasopharyngeal carcinoma in March 2015, and accepted chemotherapy after recurrence of nasopharyngeal resection in June 2015 without surgical treatment
A 58-year-old woman underwent radical radiotherapy for nasopharyngeal carcinoma in March 2015, and accepted chemotherapy after recurrence of nasopharyngeal resection in June 2015 without surgical treatment Sagittal computed tomography image indicating the region for type Ⅰ surgery(箭头所指区域)
Sagittal computed tomography image indicating the region for type Ⅰ surgery(箭头所指区域)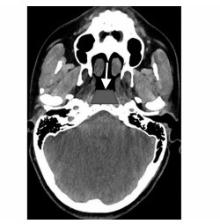 Axial CT image indicating the region for type Ⅰ surgery (箭头所指区域)
Axial CT image indicating the region for type Ⅰ surgery (箭头所指区域)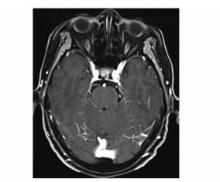 Enhanced magnetic resonance imaging indicating the disease in the midline of the nasopharynx
Enhanced magnetic resonance imaging indicating the disease in the midline of the nasopharynx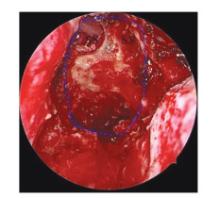 Contouring (blue dots) of the sphenoid sinus (ss) and nasopharynx
Contouring (blue dots) of the sphenoid sinus (ss) and nasopharynx| First page | Prev page | Next page | Last page | Page1 of 11, 203records |
